Bangladesh:
Concern Worldwide’s Child Survival Program
Concerted and ongoing effort is necessary at every level if child undernutrition is to be comprehensively tackled and ultimately eliminated.
Note: This case study by Concern Worldwide reflects the views of this organization. It is intended not to present research findings, but rather to show examples from their practical work and experiences in the field.

More than 10 years ago, Concern developed a program to improve maternal and child survival in Saidpur and Parbatipur, two large upazilas (or, municipalities) in northern Bangladesh. The program set out to achieve its goal by empowering individuals and communities to understand and adopt caring practices essential to the survival of children and mothers.
These practices included seeking health services such as immunization and treatment at the first sign of illness. They thus increased the demand for high-quality health services within the municipalities. At the same time, the program sought to harness the power of networks at the local level to manage and implement their own health services thereby ensuring that health services were available and accessible to those seeking them.
These efforts were undertaken within the existing policy framework, which called for the creation of municipal and community-level health committees, but these were not yet in place at the time. The program recognized this gap between policy and practice and the fact that urban slum communities had very few functioning health services. The new approach marked a bold shift from Concern’s previous focus on direct provision of health services, with very specific consideration and importance given to a rights-based approach to health (see box on page 36).
Although explicitly focused on health, the program also emphasized the importance of nutrition, beginning with the recognition that child survival depended on ensuring good nutrition practices, particularly optimum breastfeeding and vitamin-A supplementation. At the same time, by working to improve access to health, water, and sanitation services, and caring practices and resources for women and children, the program tackled two of the key underlying causes of undernutrition.
In this way, the program sought to extend its impact beyond basic survival to support the physical and mental development of children through improved nutrition (see box below).
Child nutrition in Bangladesh
Over the past 25 years, Bangladesh has made significant progress in reducing its under-five mortality rate and the prevalence of both underweight and stunting. Despite improvement, 54 of 1,000 children do not survive to their fifth birthday, while a staggering 43 percent of Bangladeshi children are stunted. With a population of 160 million, Bangladesh is one of the most densely populated countries in the world. Because of its large population, the country is home to almost 4 percent of the world’s stunted children (UNICEF 2009b).
The leading causes of death in the country are neonatal disorders (48 percent), followed by diarrhea (20 percent), pneumonia (15 percent), and other diseases and causes (17 percent). It is now known that maternal and child undernutrition is responsible for 35 percent of the global under- five death burden, and it is likely that Bangladesh is no exception.
Urbanization is occurring at an alarming rate. Almost 30 percent of the population now lives in urban areas. Although some statistics show that health services are more accessible in urban centers, these figures often mask the enormous chasm between higher and lower economic classes. Urban slums present particular threats to child survival, and the three underlying causes of undernutrition and child death – inadequate access to food, insufficient care for women and children, and inadequate access to healthcare and an unhealthy environment – present a constant challenge to the survival and development of the children of the urban poor.
The Right to Adequate Food and Nutritional Health
At the World Summit on Food Security in 2009, UN Member States reaffirmed “the right of everyone to have access to safe, sufficient and nutritious food, consistent with the progressive realization of the right to adequate food in the context of national food security.”
The right to adequate food is a human right laid down in international legal human rights conventions, together with other rights conducive to food security and nutritional health. The majority of UN Member States have ratified these conventions and are thereby bound to implement their content.
An increasing number of states, international organizations, and civil society have begun to explore a rights-based approach to development efforts, including activities promoting food security and nutritional health. They recognize that merely increasing food production will not end hunger and malnutrition and that those who are poor, hungry, or undernourished must get access to food.
Who and where they are must first be identified, and the causes of their situation fully understood and exposed. Vulnerable and marginalized groups can then be specifically supported by agricultural programs facilitating their ability to feed themselves or social protection schemes ensuring that no individual in need is left out.
A human rights-based approach to such programs and schemes necessitates strict adherence to certain principles in their implementation. Some of those principles are already generally accepted in development language, such as transparency, empowerment, and participation, while human rights also require respect for human dignity, non-discrimination, a high request for accountability, and respect for the rule of law.
"Adequate food" entails not only sufficient quantity, but also dietary diversity to satisfy nutritional needs, food safety, and compliance with cultural food values. These attributes have traditionally not received proper attention in food security policies and programming. Hopefully new political commitments and initiatives will emerge from governments of food- and nutrition-insecure countries toward policies and programs conducive to the realization of the right to adequate food, fully supported by donors and NGOs alike.
Authoritative interpretations and guidelines are available to assist interested actors in operationalizing the right to adequate food in context. See especially here and here.
Source: W. B. Eide
Example of Child Growth Cards Used in the Child Nutrition Programs in Bangladesh:
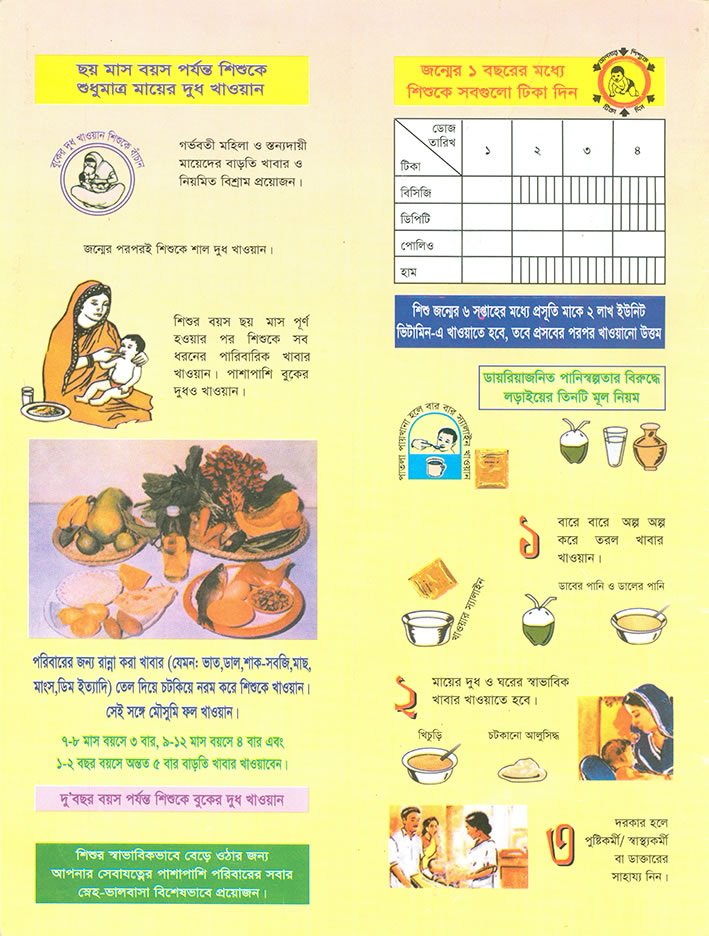 Health education messages on breastfeeding, complementary feeding, home management of diarrhea, child immunization, etc.
Health education messages on breastfeeding, complementary feeding, home management of diarrhea, child immunization, etc.
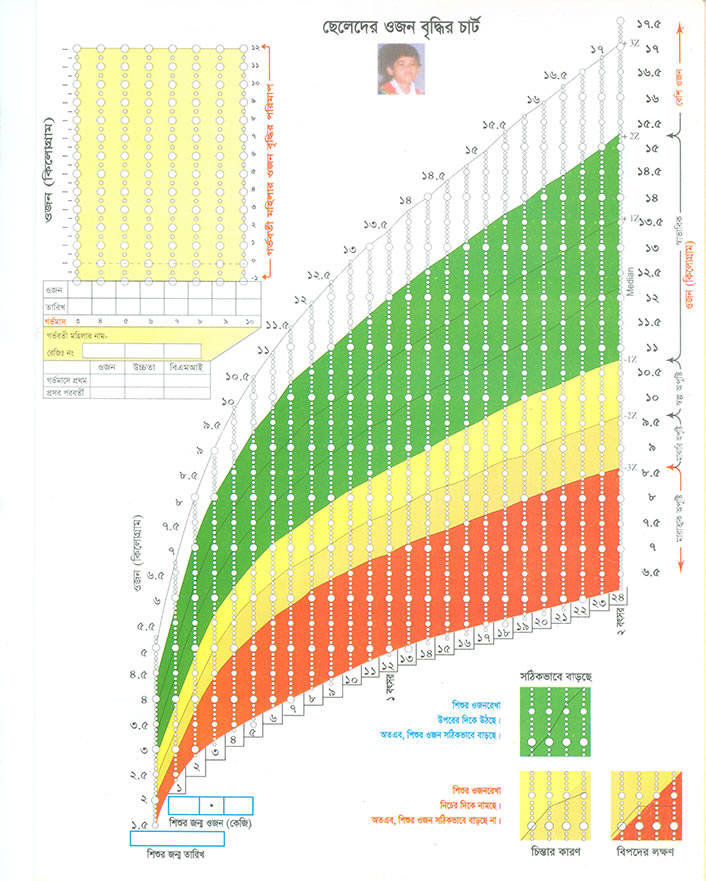 Growth chart to identify obesity, normal weight, mild, moderate and severe malnutrition.
Growth chart to identify obesity, normal weight, mild, moderate and severe malnutrition. Mothers’ meeting at the Maternity Health Ward, Rangpur, Bangladesh.
Mothers’ meeting at the Maternity Health Ward, Rangpur, Bangladesh.Sowing the Seeds: Empowering Communities and Improving Knowledge
The first step in empowering communities was to engage municipal leaders, including mayors and councilors, in establishing municipal and ward health committees. The program achieved the buy-in and participation of community leaders – crucial to the formation of these committees – through information sessions and dialogue on the existing policy framework, which outlined the roles and responsibilities of municipal authorities in implementing and managing health services. This effort was particularly important in the urban Bangladesh context. Once recruited, committee members were oriented on how best to manage their responsibilities, to obtain central-level funding, to support and supervise volunteers, and to monitor program activities and outcomes.
Community health volunteers, in turn, were trained on key health practices, including the danger signs and management of child illness, safe motherhood, newborn care, and nutrition. Each volunteer was assigned to work with 20–25 households, encouraging and supporting mothers to adopt positive health practices, referring patients to health facilities, and collecting community-level information to monitor the program. The program also provided training to community birth attendants to refer expectant mothers at the first sign of danger and to facilitate transport to hospitals.
Results after the first five years of the program (1999–2004) showed improvements in coverage of vaccination and vitamin A supplementation as well as other indicators. Based on these positive results, the program was scaled up across a further seven municipalities between 2005 and 2009, and the two original program sites were used as learning centers. Over a decade, the program reached approximately 1 million people across nine regions.
Signs of Success: Improved Uptake of Key Health Services and Practices
There are strong indications that the uptake of key maternal and child health services and practices has improved across the expanded Child Survival Program area, according to the results of surveys conducted at the start (2005) and end (2009) of the program across seven municipalities (see page 38). The largest change occurred in the coverage of vitamin A supplementation for young children and postpartum mothers. Additional, though less dramatic, improvements can be seen in other indicators. Overall, the trend is positive, but the variation in results points to the fact that cultural and access-related barriers likely still need to be overcome if mothers and communities are to adopt improved practices at scale.
Lasting Results: Signs of Continued Empowerment and Improved Knowledge
Sustaining positive health and nutrition outcomes over time – after the formal program period is over – is often the most challenging aspec of any intervention. One year after the formal completion of the Child Survival Program, a visit was made to the program area to talk with communities. Their reflections bring to life the legacy and the lessons of the program. Although clear signs of continued empowerment and improved knowledge among mothers, community health volunteers, and community leaders are evident, there are also some reminders of the challenges households continue to face when striving to put optimum health and nutrition behaviors into practice.
One of the mothers who took part in the program said:
“We can recognize the sign of malnutrition, such as if a child loses weight, their hair or skin color changes, or they become irritable. We know about types of foods. When you come across a malnourished child, the foods should be, for energy, rice, bread, and potatoes; for protein, fish or dhal (beans). Yellow fruits and green vegetables are good sources of vitamins.”A community birth attendant explained how practices had changed:
Before we did not know how to conduct a safe delivery, we would do it on the floor with no clean surface. Now we use a clean surface and know about our own hygiene and nails. When we received training we learned many ideal practices; we could see that practices in the past were not best and that helped change our perception.
Community volunteers demonstrated their knowledge and continued role in the community after the program:
We feel proud because so many people know us and know about our social activities... Even though the project has ended, they still know us and know that we have knowledge, and they continue to seek us out for help.
Improved knowledge extends to the ward health committees as well, whose members discussed appropriate feeding practices with accuracy and also spoke of their wider sense of responsibility.
Before we were not knowledgeable, and we were not involved in anything other than national initiatives. Now we are involved, we have an exchange of information between groups, and the ward health committee is well defined. We have a ward map which shows the location of all households, of the committee members, of the volunteers, and the community birth attendants. We have a picture of our community and where the resources are, and we know how to mobilize them. Mothers now know where they can receive healthcare services; even if they cannot afford to pay, they know where there is a free clinic.
The engagement and involvement of community leaders in the program ensured a sense of ownership and common purpose with regard to improving access to healthcare. One mayor explained:
Before, the role of the municipality was [simply] facilitating immunization and overseeing birth records. Now I see my role in a different way. For example, before if a pregnant mother needed to have a Caesarean section and it was the evening or a time when Caesareans were not done, the mother had to wait, and the mother and child both suffered. We have ensured that the government facilities are now available 24/7. I have a vision that no one should die because of a lack of healthcare.
The ward health committees continue the work they began in 2005. They provide funds for those who cannot afford healthcare in case of an emergency. One committee member explained:
If a family has a health emergency, and they don’t have the money, the ward health committee comes forward to support them and the volunteers or birth attendants will accompany them to the health facility.
The committees continue to organize health events, motivate and support volunteers, and collect information on their areas. Community volunteers and birth attendants refer and accompany mothers and sick children to healthcare facilities. The municipal cabinets ensure that the community health volunteers and birth attendants have easy access to hospitals and clinics and have all types of support when they refer a patient.
Volunteers and birth attendants are each issued identification cards by the municipality.
Community members trust the volunteers’ knowledge because it has proven to be correct and often lifesaving over time. One volunteer said confidence in the volunteers grows when she diagnoses a child with respiratory infection, when this diagnosis is confirmed by the health facility, and when the mother sees the child recover after treatment.
The Child Survival Program began with a nonfunctioning health system that only supported national immunization days. It left in its wake a trained, motivated workforce and increased access to healthcare by mothers. It is a huge step in the direction of reducing child undernutrition, and evaluations have shown a range of positive changes.
By leveraging existing resources within communities, working with governments to create a more favorable environment for healthcare, and providing the necessary education and range of support mechanisms, mothers were empowered to take better care of their infants and young children. Strong monitoring and evaluation have allowed this impact to be measured and learning to be consolidated for future programs. One community health volunteer explained:
The members of the community know us, the volunteers. They did not know Concern. Even though the project has ended, they still know us and know that we have knowledge, and they continue to seek us out for help.
In 2009, an assessment was conducted to determine the sustainability of the 2000–04 program. This assessment found that although external inputs fell to almost zero, the municipalities were able to maintain basic operations and improve many health indicators.
Though the assessment identified some gaps, it more broadly confirmed the lasting value of an urban health model resting on the municipal government and ward health committees. The assessment led to a set of recommendations that were made to municipalities and stakeholders so they could focus on the areas of greatest challenge and continue to build on the foundations laid.
The results of both programs, and the reflections on them, show the changes and challenges that exist at the community level and illustrate the kinds of success and learning that are possible, and indeed necessary. Set against the backdrop of the wider analysis of the Global Hunger Index, these studies also show the concerted and ongoing effort that is necessary at every level if child undernutrition is to be comprehensively addressed and ultimately eliminated.