Community Perspectives on Early Childhood Undernutrition in Mali
Welthungerhilfe’s Program for the Promotion of Best Practices in Agriculture, Nutrition, and Health
Note: This case study by Welthungerhilfe reflects the views of this organization. It is intended not to present research findings, but rather to show examples from their practical work and experiences in the field.
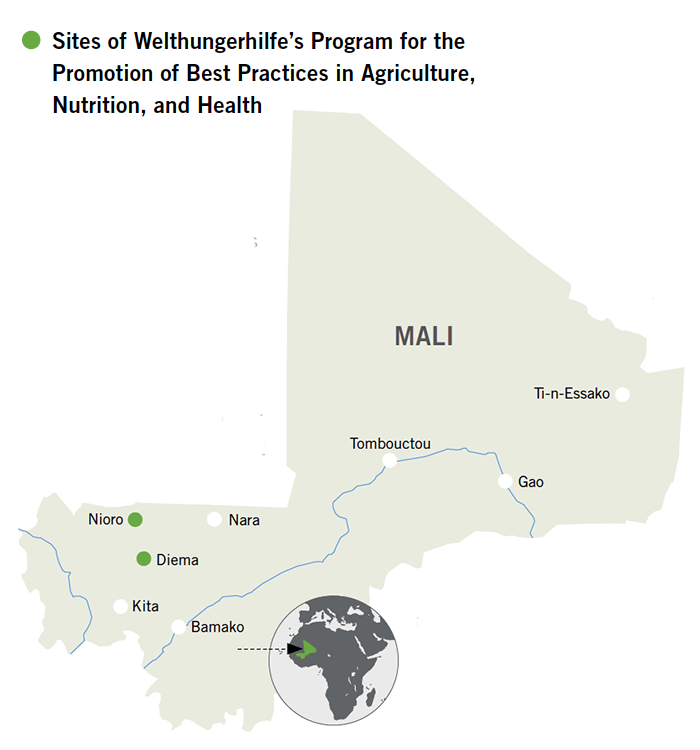
Welthungerhilfe has worked in Mali since 1968. It currently supports the Program for the Promotion of Best Practices in Agriculture, Nutrition, and Health in 100 particularly food-insecure villages in the two districts of Nioro du Sahel and Diema, in the Kayes region near the border with Mauritania. The four-year program, which runs from 2008 to 2011, is designed to benefit approximately 125,000 people. Its overall aim is to contribute to improving the nutritional status of children under five and pregnant and lactating women and to enhance the food security of vulnerable populations. Specifically, the project aims to reduce the prevalence of chronic childhood undernutrition in the area by 50 percent (see box below).
A representative baseline survey (using a clustered random sampling method) was conducted in the intervention area before project activities commenced (March–May 2008). The survey showed that stunting levels in the target area (37 percent) were very close to those seen nationally. The survey also showed that health and nutrition practices were suboptimal. Some water and foods were being introduced before the age of six months, while complementary foods were introduced later than six months; feeding frequency once complementary foods were introduced was also low. Mothers themselves were found to be undernourished (18.1 percent were underweight with a BMI < 18.5, and an additional 23.5 percent were at risk of being underweight with a BMI < 20) with a low level of education (1.4 percent were literate; 67.9 percent had no education).
It was also found that children were frequently ill; 32 percent were sick during the two weeks before the survey and 32 percent of children surveyed drank regularly from unprotected water sources. Access to health services was limited, and it was found that more than half (55 percent) of pregnant women had not had any sort of antenatal visit. There is a seasonal “hunger gap” that begins once the annual harvest is consumed and before the next arrives. Yearly rainfall averages between 300 and 550 millimeters and usually comes in a concentrated stretch between July and October, followed by a long, dry postharvest season. Millet and sorghum are the main crops, with some farmers growing smaller plots of groundnuts and cowpeas.
Welthungerhilfe initiated its project to address these problems in an integrated manner, fostering improved health and nutritional knowledge and practice while supporting increased agricultural productivity and enhancing the capacity of existing communal structures to manage and maintain those improvements.
After two years of implementation, communities in the program area noted changes that, in recent discussions, were attributed to the project.
Improving Care for Women and Children
Child Nutrition in Mali
More than one-third (34 percent) of Mali’s children are stunted, and one in 10 (11 percent) suffers from wasting. Even more stark is the fact that there has been no improvement in either statistic over the past decade and a half – stunting levels were basically the same in 1996 (33 percent) as they are now, and since then the prevalence of wasting has more than doubled (from 5 percent in 1996) (UNICEF 2003–08).
Mali, a landlocked country in West Africa with an estimated population of 13.5 million (Samaké 2007), is one of the poorest countries in the world. In 2006, more than half of the population was living on less than US$1.25 a day and more than 70 percent on less than US$2 a day. More than two-thirds of the population lives in rural areas, and the vast majority of the population (approximately 80 percent) works in agriculture (République du Mali 2005).
As in much of the Sahel, depending on agriculture for one’s primary livelihood is a risky endeavor in Mali. In the absence of irrigation systems, most crops are dependent solely on rainfall. That rainfall is generally limited and inconsistent. As a result, dramatic fluctuations in annual agricultural production are the norm, and families, particularly children, are at risk of suffering as a result of these shortfalls.
Seasonal locust and granivore infestations compound the effects of drought, and the result can be crippling for the average farming household. Such was the case in 2004, when poor harvests across the country led to a severe food crisis in 2005. A similar crisis unfolded in northern Mali in early 2010 following unusually low rainfall the year before. A drought appeal was launched, and the emergency response continued throughout 2010 although some would argue such emergency measures are often “too little, too late.”
The underlying causes of undernutrition all exist in Mali. Pervasive poverty and high food insecurity exist alongside limited access to healthcare, water, and sanitation services, and maternal and child caring practices are suboptimal in many areas. In a national survey in 2006, the majority of rural women (72 percent) cited major barriers to gaining access to healthcare, the most common being a lack of money (59 percent), followed by distance to health centers (48.2 percent) and lack of transportation (42 percent) (Samaké 2007).
Initial assessments determined that health promotion at the community level was weak but that some dormant community health volunteers did exist. While a cadre of volunteers had been trained previously, most were no longer active because of lack of follow-up support. Building on this existing capacity, the project identified and reactivated these volunteers by providing refresher training on a wide range of nutrition- and health-related topics and providing supportive supervision through the project’s health advisers.
Changing feeding habits in northwest Mali is a challenge. Families have strong traditional beliefs that babies should be fed animal milk, and women have a very low level of education. In this context, it proved critical to train community health volunteers not only in the key messages, but also in how to speak with people. All volunteers received training in interpersonal communication, the qualities of a good facilitator, and how to conduct educational discussions, counseling, and home visits. To reinforce the messages of the community health volunteers, the same key messages were broadcast by radio in the local language.
There are indications that mothers in the project area are adopting improved practices based on the messages and counseling they are receiving from volunteers. One mother said she had abandoned the traditional practice of discarding the mother’s first milk, the nutrient-dense colostrum, and had moved toward exclusively breastfeeding and improved complementary feeding for her most recent child:
Now for the first six months we only give breast milk. Before, the first milk given to a newborn was goat’s milk; now we give mother’s milk first. The volunteer has explained that if we look at animals, such as goats, cows, and horses, we see that they give the first milk to their newborns. If other animals give the first milk, it must not be poison... Before, we did not know how to make appropriate foods with locally available products; when we were eating we would just give a portion [from the adult’s plate] to our child. I have seen a change from the birth of my [youngest] child until now since I was counseled. She received breast milk for the first six months and was fed appropriately after that. I can see a difference from my previous child. Since her birth my youngest child has not fallen sick.
The volunteers also conducted cooking presentations using recipes based on locally available foods, providing for a balanced diet.
Improving access to healthcare
Increasing the knowledge of health volunteers was the first step toward ensuring that undernourished children receive the appropriate treatment, as one of the project’s health advisers explained:
In the training we showed pictures of children with different types of malnutrition, including kwashiorkor, marasmus, and edema. We used pictures of children from the area. They had never seen pictures of malnourished children before. At first volunteers did not believe they were malnourished or did not believe the children were from the area.
And a volunteer confirms: “We did not know the signs. Now we see that it is a problem, and we know how to address it.” In order to ensure that mothers of malnourished children can overcome barriers to gaining access to healthcare, community nutrition funds were established from money contributed by households and matched by the project. The fund is managed by a community committee and is kept in a local banking facility. One mother spoke about the fund in her village:
We now have a community nutrition fund. If a child is sick and the community health staff refers him to the center in Nioro, we take money from the fund for the transportation of the child.
By January 2010, community nutrition funds had been established in 48 villages, and 1,583,075 CFA francs (about US$3,130) had been raised. The staff at the public health centers confirmed that more community members are using the centers, with a particular increase in the number of undernourished children being referred. This suggests that more children are being treated.
Improving access to quality foods
Increased knowledge of feeding practices and healthy diets can make a difference only if there is sufficient access to food. The initial baseline study identified inconsistent rain, poor soil quality, erosion, and poor quality of seeds as key barriers to ensuring levels of agricultural production that would close the seasonal “hunger gap.”
Based on a further study that looked at the needs and available resources in each village, a variety of food security, agriculture, and community capacity-building activities were implemented in the program area. Training was carried out for heads of households on erosion control methods including construction of check dams, seed improvement, and seed multiplication. The aims were to maximize production of rainfed plots and to encourage diversification of crops. These activities were combined with training in correct storage, especially during the dry season. The project also supported the formation of women’s garden associations and the construction of wells.
Though initially skeptical, farmers were soon convinced by the early successes and began to engage in further program activities.
In the first year, we only sowed a small portion of the new seeds. We saw how much better it worked and did larger amounts in the second year... Now this year there are some that are only using the new seeds. The new seeds produce around 500 kilos for every 1 kilo of seeds. The old seeds only produced around 300 kilos... Before, the level of production of beans was so low that we only had enough for part of the year. Now households have enough beans to last the whole year.
This initial trust and confidence are critical to the next step, which is to work with farmers to expand replication of their own and improved seed varieties to replenish their stocks.
Training for the members of the garden associations led to increased diversity of food produced, eaten, and sold. One village woman reported:
We grow a wide variety of vegetables including onions, cabbage, tomatoes, carrots, and eggplant. Before, we only knew about lettuce and onions... The first portion that we harvest is eaten, but if the production is large, then we sell a proportion to add to our savings. The project built one large well and two small wells in our village. We do not have to go to the neighboring village to get water anymore. Even now in June, there are some that are still gardening.
After two years of implementation, 289 women gardeners had been trained in vegetable drying and conservation techniques in order to improve access to diversified foods throughout the “hunger gap” period.
Through small steps, the project has made considerable contributions to household income and food security.
Enduring Challenges
Two years into the project, Welthungerhilfe understands some of the challenges to achieving sustained impact and scaling it up and is working to find solutions based on that understanding.
One challenge results from the fact that the agricultural calendar requires labor for sowing and weeding crops just as farmers in Mali are experiencing the “hungry season.” Community health volunteers, who are farmers themselves, find it difficult to carry out their responsibilities during this period. As one volunteer explained:
Everyone has a lot of work to do during the day, and at night they are tired and sleeping, making it difficult to visit households to deliver health messages and check for illness.
Thus, the monitoring of children’s health and nutritional status is especially difficult during the period when it is most necessary. The program addresses this challenge by promoting compensation schemes for the volunteers, which are managed by the communities and enable the volunteers to seek assistance for the field work.
Another challenge is the longer-term sustainability of interventions. The project has successfully engaged the local population – farmers, mothers, and other communal stakeholders – and helped them identify with the intervention as they acknowledge improvement in their daily lives. Public authorities are systematically participating in the planning and monitoring of all interventions, and all project activities are integrated into communal strategies for ecological, social, and cultural development. Nevertheless, it may prove difficult for local authorities to uphold their commitments once the external support phases out, given the limited support from the regional and national levels.
The reflections provided by volunteers and community members suggest that the program has taken the right approach by comprehensively aiming to increase knowledge on health and nutrition, improving access to healthcare, and addressing issues of food availability. A final program evaluation will be undertaken to verify the extent to which the increased knowledge among volunteers and community members leads to sustainable behavioral changes and thus reductions in child undernutrition rates.
Footnotes
- Welthungerhilfe is grateful for the European Commission’s financial support for this program.
- This diagnostic study was conducted by the local nongovernmental organization (NGO) partner Association pour l’Appui au Développement Global, or Association for the Support of Global Development (ADG). It consisted of a review of available literature and working sessions with a variety of stakeholders, including elected officials and villagers. Participatory tools were used. For each village, the study outlines the location, climate and vegetation, demographics, potential for and constraints of food production, existing projects, and community organizations, as well as the basic problems and constraints faced.
About this Case Study
This case study provides insight into a Welthungerhilfe project in rural Mali. In June 2010, Sally Newman Abbott, an external consultant, visited the program area to interview local stakeholders on their personal views of the problem of early childhood undernutrition as well as on the changes and limitations they observe.
These reflections, gathered in preparation for the Global Hunger Index, are from people who are directly affected by child malnutrition: mothers, community workers, and local leaders. They give voice to those who face the daily challenges of trying to ensure good nutrition for mothers and children.