Fighting the Crisis of Early Childhood Undernutrition
The Thousand-Day Window of Opportunity
Children who are undernourished during the thousand-day window risk experiencing lifelong damage, poor health, and even early death.
Note: The views expressed in this chapter are those of the author. They do not necessarily reflect the views of IFPRI, Welthungerhilfe, or Concern Worldwide.
The Global Hunger Index includes three components (proportion of undernourished, prevalence of underweight children and under-five mortality rate). The world GHI score is 15.1: child underweight contributes up to 7.4 points, or nearly half of the score, whereas the proportion of undernourished and under five mortality contribute 5.4 and 2.2 points, respectively. In South Asia, underweight in children under five accounts for more than half of the GHI score of 22.9. In Sub-Saharan Africa, the situation is slightly different. There, the GHI score has barely improved over the past 20 years, and underweight in children under five has improved only slightly, falling from 27.2 to 23.6 percent, according to recent estimates. In order to improve their GHI scores, countries need to accelerate progress in reducing child underweight by improving childhood nutrition.
How can this be done? The first step is to focus on the age group of children that represents the window of opportunity for improving nutrition. Although past policies and programs targeted children under the age of five for nutrition interventions in many countries, recent evidence clearly shows that the window of opportunity for improving nutrition is much narrower, spanning the period from -9 to +24 months (that is, the 1,000 days between conception and a child’s second birthday). This is the period not only when children are in greatest need of adequate amounts of nutritious food for healthy development, but also when interventions are most likely to prevent undernutrition from setting in.
After the age of two, the effects of undernutrition are largely irreversible (Ruel 2010). Children who are undernourished during the thousand-day window risk experiencing lifelong damage, including poor physical and cognitive development, poor health, and even early death. These children are likely to grow up to be short and thin, as well as less productive and healthy than they might have been. Furthermore, when poorly nourished girls grow up, they tend to give birth to underweight babies, perpetuating the cycle of undernutrition. This means that the well-being of mothers is a critical element of the solution.
The ingredients of proper early childhood nutrition are well known: a well-nourished and empowered mother who has good nutrition and health before and during her pregnancy; who receives adequate health support and care to ensure a safe delivery for herself and her newborn baby; who breastfeeds exclusively for the first six months of the infant’s life and continues breastfeeding until at least two years of age; who provides the infant with nutritious complementary foods in adequate quantities and frequency starting at six months of age; and who has access to safe water, sanitation, and preventive and curative healthcare. Yet millions of people lack these basic ingredients.
A Global Crisis of Child Undernutrition.
ALL CHILD UNDERNUTRITION IS NOT THE SAME: THE FORMS OF POOR NUTRITION
Child undernutrition can manifest itself in different ways, depending on the cause, severity, and duration. The three main measures of child undernutrition are:
- stunting – low height for one’s age,
- wasting – low weight for one’s height, and
- underweight – low weight for one’s age.
Stunting is a good overall indicator of undernutrition because it reflects the cumulative effects of chronic undernutrition. Wasting reflects acute undernutrition resulting from inadequate food and nutrient intake and/or repeated or severe disease. Underweight reflects either stunting or wasting, or both.
Researchers measure these indicators using Z scores. These scores reflect how much a child’s weight or height deviates from the standard for healthy child growth set by the World Health Organization. The closer a child’s Z score is to zero, the closer he or she is to the median of the international growth reference standard. This standard is based on the fact that children of all races and ethnicities have the capacity to reach a healthy weight and height. In 2006, the World Health Organization updated its child growth standards, showing that global child undernutrition was even more severe than previously thought. For all three indicators, undernutrition (as represented by stunting, wasting, or underweight) is defined as a Z score below -2 and severe undernutrition as a Z score below -3.
Another form of undernutrition consists of deficiencies of essential micronutrients – vitamins and minerals, especially iron, iodine, zinc and vitamin A. Deficiencies of micronutrients are also referred to as “hidden hunger” because they are often present without showing any clinical signs. In the absence of blood tests, they may remain undetected until they become very severe and life-threatening. Micronutrient deficiencies can have devastating effects in women and young children and can affect child growth, motor and cognitive development, resistance to infections and survival. In women, micronutrient deficiency can reduce their ability to have a safe pregnancy and delivery, produce breast milk in sufficient amounts and quality and remain healthy.
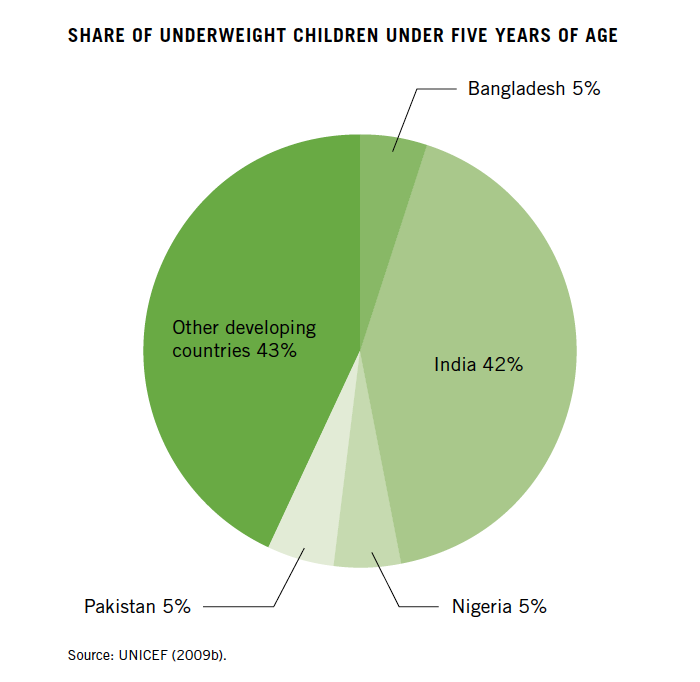
Child undernutrition has reached epidemic proportions. Stunting affects about 195 million children under the age of five in the developing world – about one in three children. Nearly one in four children under age five – 129 million – is underweight, and one in 10 is severely underweight (UNICEF 2009b; see box right).
Child undernutrition is not spread evenly across the globe but is instead concentrated in a few countries and regions. More than 90 percent of the world’s stunted children live in Africa and Asia, where rates of stunting are 40 percent and 36 percent respectively (UNICEF 2009b). Indeed, more than 80 percent of the global burden of child undernutrition (as measured by stunting) occurs in just 24 countries.
India alone accounts for a large share of the world’s undernourished children. In 2005–06, about 44 percent of Indian children under age five were underweight and 48 percent were stunted (WHO 2010b). Because of the country’s sheer size, these numbers mean that India is home to 42 percent of the world’s underweight children (see figure above right) and 31 percent of its stunted children (UNICEF 2009b).
High levels of child undernutrition are also found in several other South Asian and African countries. In some countries of Sub-Saharan Africa, about half of all children are stunted: 53 percent of children in Burundi, Madagascar, and Malawi are stunted; in Ethiopia and Rwanda, the figure stands at 51 percent; and in Guinea-Bissau and Niger, at 47 percent (UNICEF 2009b). More than half of under-five children in Afghanistan, Guatemala, Timor-Leste, and Yemen are also stunted.
Micronutrient deficiencies, which can result in so-called hidden hunger because their effects are often not visible, are even more widespread than underweight, stunting, and wasting. Globally, about 2 billion people suffer from iodine deficiency, including 285 million children aged 6 to 12 years (de Benoist et al. 2004). Almost 50 percent of children age five and under have anemia, about half of which is caused by iron deficiency (de Benoist et al. 2008). The greatest share of preschool children suffering from anemia – 68 percent – is in Africa. Vitamin-A deficiencies affect 190 million preschool children (WHO 2009).
This burden of undernutrition takes a heavy toll on children’s health and survival. Researchers have estimated that stunting, wasting, and intrauterine growth restriction (which causes low birth weight) together are responsible for 2.2 million deaths a year (Black et al. 2008). Vitamin-A deficiency leads to a host of health problems, including blindness in extreme cases, and increases children’s risk of dying from other conditions, such as diarrhea and malaria.
Zinc deficiency increases children’s risk of diarrhea, pneumonia, and malaria. Iron deficiency can increase maternal mortality and lower children’s cognitive capacity. Iodine deficiency during pregnancy not only threatens the outcome of the pregnancy, but also impairs the fetus’s mental and motor development. Chronic iodine deficiency has a substantial impact on cognitive development.
The Perilous Thousand Days
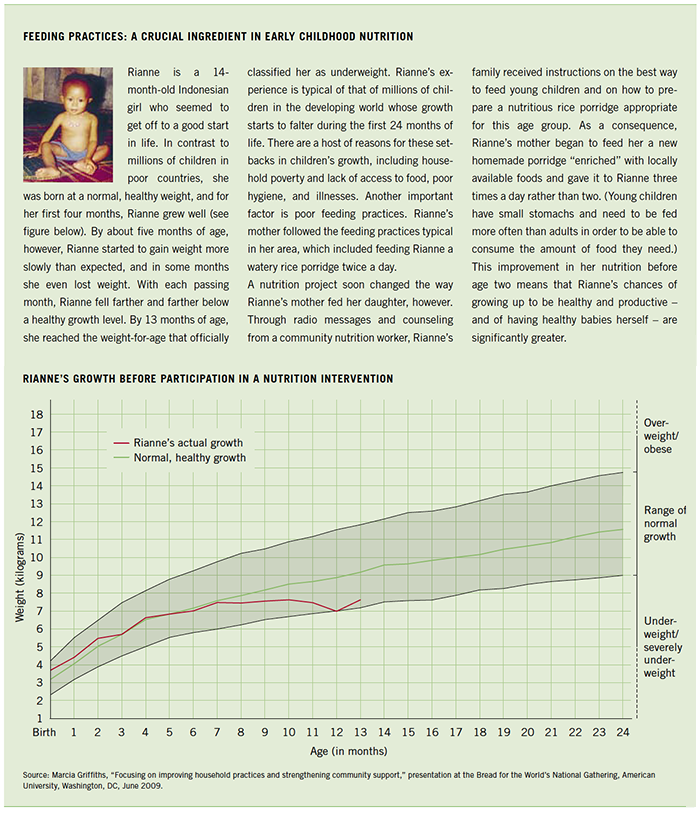
Many children in developing countries start to experience growth faltering during their first year of life, and indeed, even before they are born. Analyzing data from 54 countries in Africa, Asia, and Latin America, researchers found that the bulk of growth faltering – particularly stunting and underweight – occurs from birth to age two (see graph on top of page 23; Victora et al. 2010).
The second chart below shows that children are born at a height close to the standard in most regions, but growth begins to lag after a few months and deteriorates quickly until about the age of 24 months. Children in South Asia are worst off, partly because they start at a deficit; even at birth, many infants in South Asia are already stunted. Across the world, by the age of two years, most of the damage is done. On average these children experience little or no further deterioration, and they stabilize at low levels of weight and height for their age, with children in South Asia and Sub-Saharan Africa showing the severest rates of stunting.
Why is the period from conception to age two so critical from a nutritional point of view? To begin with, if a mother has poor nutrition before and during pregnancy, a baby is likely to be born small. Poor maternal nutrition is a particularly severe problem in Asia. In some countries in South Asia, more than 10 percent of women are shorter than 145 centimeters, a threshold that puts women at risk of having complications during delivery and of having small babies. In most countries of South and Southeast Asia, as well as in Sub-Saharan Africa and in Yemen, more than 20 percent of women have a low body mass index (Black et al. 2008).
In many of these countries, women also have low social status; they are often the last in the household to eat, and they do not receive the care they need, particularly in their childbearing years. Poor nutrition in women throughout their own life cycle thus extends through the generations: Undernourished girls become short women, and short women give birth to smaller children. This vicious circle is perpetuated by women’s low social status.
After birth, many infants may not be exclusively breastfed. Mothers may find it difficult to breastfeed exclusively because they are poorly nourished themselves or because they have a heavy workload; many are simply unaware that breast milk is all a young infant needs. Often, infants are given water, tea, or other drinks in addition to breast milk – practices that can increase a child’s risk of acquiring infections and lead to inadequate nutrient intake because they displace breast milk.
At six months, the child should be given nutritious complementary foods, but this may happen too early or too late; in some countries, children are given complementary foods at one week or one month of age (Tontisirin and Winichagoon 1999). In other countries, food is introduced well beyond the recommended age of six months. In addition, the complementary foods may be of poor nutritional quality or given too infrequently (see box right). Other families may simply not have access to enough nutritious food for their young children.
Moreover, health issues can take a heavy toll on children’s nutritional status. Where there is no access to sanitation and clean water, children may suffer from repeated infections, which can lead to lack of appetite; loss of nutrients stemming from fever, diarrhea, and vomiting; and poor absorption of nutrients. In these environments, children are also unlikely to get their immunizations and regular health check-ups.

Yat Samath,
Ratanakiri Province, Cambodia
The district health center gave me iron tablets twice (around 40 tablets in total). I took all iron tablets, also after some pregnant ladies from the village advised me not to take them. They feared that the fetus will be fat and difficult to deliver.
During my pregnancy I didn’t eat turtles and all kinds of snakes, because I was afraid that if I ate these kinds of animals, my children will become turtles.
During the first two days, my infant had extra milk to drink but it was not enough. Also I have given my breast to her, but it was dry, and she sucked without getting milk. I drank some traditional medicine to produce more milk, named ‘MemayKounMouy’.

Dr. Kyawt Thazin Oo,
Nutritionist, Irawadi-Division, Myanmar
The majority of mothers usually starts supplementary feeding before six months. The majority of supplementary food is rice and soft fruits. Children are served similar food as the adults in the family. Staple meals in the Ayerwaddy delta consist mainly of rice and traditional fish paste made of fermented fish and prawns . For very young children, mothers first chew food and then feed it to children who have not developed a full set of teeth.
The Lifelong Costs of Poor Nutrition in Early Childhood
Nutrition deficits early in life have both short-term and long-term effects that last into adulthood. Children who are undernourished in utero, during their first two years, or both are more likely to become shorter adults, complete fewer years of schooling, earn less income, and have children with lower birth weights. Developing countries can experience GDP losses of up to 2–3 percent per annum as a result of undernutrition, rising to as high as 6 percent (CEPAL/PMA 2007). One study found that Zimbabwean children who were stunted as preschoolers started school seven months later than comparable children who were not stunted, and they lost an average of 0.7 grades of schooling (Alderman, Hoddinott, and Kinsey 2003).
These delays and losses in schooling translated into a 12-percent reduction in lifetime earnings. Undernutrition in early childhood can also increase the risks of obesity and chronic diseases in adulthood. Undernourished children who gain weight rapidly in later childhood and adolescence are at higher risk of nutrition-related illnesses such as diabetes and cardiovascular diseases as adults than children who are well nourished during early childhood. Overall, it has been estimated that 11 percent of the total global disease burden is related to undernutrition (Black et al. 2008).
The Economic Benefits of Addressing Undernutrition
The interventions, both direct and indirect, that can effectively combat undernutrition are largely known. Moreover, investing in the fight against undernutrition brings high returns. In Guatemala, boys who participated in an early childhood intervention that improved their nutrition during their first two to three years of life had 46 percent higher wages in adulthood than those who did not participate in the intervention (Hoddinott et al. 2008). As part of the Copenhagen Consensus 2008, a panel of experts consisting of eight leading economists critically examined and ranked the world's biggest problems and concluded that the greatest development good would come from a nutrition intervention (the provision of micronutrient supplements for children – vitamin A every four to six months for children six months to five years old and therapeutic zinc supplementation for diarrhea).
They calculated that investments in micronutrient supplements for children yield returns of between $14 (zinc) and $17 (vitamin A) for every $1 spent (Horton et al. 2008).
Preventing Early Childhood Undernutrition
After the age of two years, the effects of undernutrition are largely irreversible. Missing the “window of opportunity” – the thousand-day period from conception to two years of age – to improve nutrition can result in long-term permanent damage (Victora et al. 2008). It is therefore critical that programs to prevent undernutrition reach mothers and young children during this period. For children who are exposed to severe conflict, shocks, or emergency situations after the age of two or for those who have not been reached by preventive nutrition interventions, addressing severe acute malnutrition and hunger beyond the age of two years is also critical and requires carefully targeted interventions focused on recuperation and treatment. However, research has shown that it is more effective to prevent child undernutrition than to treat it (Ruel et al. 2008), and therefore investments aimed at improving nutrition should focus on the thousand-day period. There is a clear window of opportunity for addressing nutrition, and after age two, this window closes rapidly.
Improving the health and well-being of millions of people in developing countries requires taking advantage of the window of opportunity – in other words, focusing interventions on addressing undernutrition in adolescent girls, women of childbearing age, and children under the age of two. Indeed, universal coverage of preventive health and nutrition interventions for children under the age of two and their mothers could reduce the burden of childhood undernutrition by 25–36 percent, improving the health and survival chances of millions of children (Bhutta et al. 2008).
To begin with, governments should invest in targeted nutrition interventions that will have a rapid impact on early childhood undernutrition. These interventions should focus on improving maternal nutrition during pregnancy and lactation, promoting sound breastfeeding and complementary feeding practices, if necessary providing micronutrient supplements (such as vitamin A supplementation and therapeutic zinc), and adopting universal salt iodization. Childhood immunization programs and the promotion of optimal hygiene and sanitation practices are also essential. In addition, parents must be taught about the appropriate feeding and care of children exposed to HIV and AIDS. These interventions will address the immediate causes of undernutrition (see chart on page 27).
Poor child nutrition stems from underlying causes related to the overall environment in which children are born and raised. Consequently, policies that deal more broadly with problems such as poverty; food insecurity; lack of education; the low status of women; and lack of access to water, sanitation, and health services are also needed in order for there to be a profound and sustained improvement in child nutrition. The importance of these broader factors is clear from the progress made in reducing undernutrition in Brazil, China, Thailand, and Vietnam. One promising approach is to integrate nutrition interventions into multi-sectoral programs that alleviate poverty, enhance food security, and improve gender equity. Programs that cross sectors, like conditional cash transfers (which provide households with cash transfers in exchange for children’s attendance at school and use of health facilities), have shown significant potential to improve early childhood nutrition during the window of opportunity (Leroy, Ruel, and Verhofstadt 2009). Programs that promote household production and consumption of nutritious fruits, vegetables, and animal source foods have also been shown to substantially raise the quality and diversity of the diets of all household members (World Bank 2007).

Francisca Champi Condena,
Pisco Province, Peru
When I have a lot of work in the fields I rarely cook. Sometimes we don’t have enough money to buy milk, cheese, and eggs. The harvest suffices to provide our families with enough food, but the food isn’t well balanced anymore. Vegetables, for example, we only have during the rainy season. We were taught that feeding our children cheese would cause problems with learning to speak. But I don't care about this warning. In the trainings they told us that we can feed them cheese regularly. I did so and my children are able to speak.

Tatiana Medina Sánchez,
Cajamarca Province, Peru
Little by little the nutrition of children is improving due to the interventions of NGOs and municipalities. But some families don’t improve their nutrition practices, because they dedicate more time to commercializing their agriculture or other activities. Others still aren’t used to the consumption of some particular foods.
The inhabitants of some communities don’t consider child malnutrition a priority problem. Their requests for the participative budget show that they don’t focus on tackling malnutrition.
Striking Successes
For many countries, the goal of improving early child nutrition has not yet made it onto the policy agenda, but a few countries have been able to quickly and effectively reduce child undernutrition. Although each country must design policies and programs to fit its own context, these countries’ experiences point to policy options and offer useful lessons.
Thailand, for example, halved child malnutrition from 50 to 25 percent in less than a decade during the 1980s. The country achieved this remarkable success by using targeted nutrition interventions to eliminate severe malnutrition and by creating a widespread network of community volunteers to help change people’s behavior to prevent mild to moderate malnutrition. These volunteers, who reached a ratio of 1 for every 20 households throughout Thailand, received extensive training so that they could monitor children’s growth, educate caregivers about the best ways to breastfeed and conduct complementary feeding, offer prenatal care, and provide other basic health services.
The Thai government took the view that investments in nutrition are not welfare, but rather investments in development, and it integrated nutrition into its National Economic and Social Development Plan (Tontisirin and Winichagoon 1999). At the same time, it invested heavily in health, sanitation, and education during this period.
Between 1990 and 2002, China also reduced child malnutrition by more than half, from 25 to 8 percent, with a highly successful poverty alleviation strategy; effective large-scale health, nutrition, and family-planning interventions; and increased spending on water, sanitation, and education (Ruel 2008). These investments appear to have helped improve a number of factors that are root causes of child undernutrition, including mothers’ nutritional status, the birth weight of children, maternal literacy and access to healthcare, and reduce fertility rates and poverty (Svedberg 2007).
Another success story recently unfolded in Brazil, where the prevalence of child stunting fell from 37 percent in 1974–75 to 7 percent in 2006–07. The country had a period of rapid economic growth and poverty reduction from 1970 to 1980, but the improvements in child malnutrition did not take place immediately. In the late 1970s and 1980s, however, Brazil’s social spending rose significantly, including spending on food and nutrition programs, health, and education. Coverage of safe water and child immunizations also increased dramatically (Ruel 2008). From 1996 to 2007, much of the improvement in child nutrition was due to more maternal schooling, greater family incomes, improvements in maternal and child healthcare, and better coverage of water supply and sanitation services.
Brazil’s conditional cash transfer program (Bolsa Familia) is one example of a successful poverty-alleviation program that integrates nutrition, health and education goals and interventions (Leroy, Ruel, and Verhofstadt 2009). This program and other Brazilian Government policies have also done a great deal to reduce inequality, with the result that the nutritional status of poor children has rapidly approached that of wealthier children (Monteiro et al. 2009; Monteiro et al. 2010).
At the local level too, programs have succeeded in addressing both the immediate and the underlying causes of child undernutrition: examples include gender-focused programs promoting homestead food production in Bangladesh (Iannotti, Cunningham, and Ruel 2009). Many of these programs not only incorporate direct nutrition interventions, but also work to alleviate poverty and food insecurity and to reduce gender inequality by providing women with training and resources.
Addressing the Crisis

Haja Adam Mohamed,
North Dafur, Sudan
We would like to feed our children better, but because of lack of income and high prices of cereals, we don’t have the possibility to do it. Sometimes even the lactating and pregnant women don’t have enough kilocalories as to produce enough breast milk for their babies.

Phorn Moern,
Ratanakiri Province, Cambodia
I eat only mashed chili with salt and bamboo shoots. Sometimes, when we have money we buy some fruit, chicken eggs, duck eggs, and meat from the market . To get the food we have to walk one hour, because around our village food from the forest is disappearing.

Rodine Norosea,
Nutrition technician, Fianarantsoa Province, Madagascar
The usual food consists of too many carbohydrates because of the abundance of rice they are eating. Frequently it’s not possible for people to follow our recommendations and recipes, because the required food isn’t available or they don’t have enough money to buy it. Single mothers with many children and not enough food very often favor their older children when distributing food so that there is little left for the youngest.
The importance of nutrition is being increasingly acknowledged. It is at last inching its way up the international development agenda. The Millennium Development Goals (MDGs) have drawn attention to nutrition by focusing on halving the proportion of hungry people. The Copenhagen Consensus in 2008 declared that investments in nutrition initiatives were the most effective development investments in terms of cost and benefit.
Several new initiatives are focusing specifically on nutrition from multiple perspectives. A group of nutrition actors, representing a range of stakeholders, has issued a set of recommendations for global and national action called “Scaling Up Nutrition: A Framework for Action” (Bezanson and Isenman 2010). This document endorses a package of nutrition interventions targeted toward the window of opportunity and estimates the costs of scaling up these interventions from current levels to the levels needed to achieve rapid reductions in undernutrition.
In addition, based on discussions following the global food, fuel, and financial crises, the Group of Eight industrial countries agreed through the L’Aquila Joint Statement on Global Food Security to place new emphasis on food security and nutrition in poor countries. Building on this statement, multiple donors have contributed to the Global Agriculture and Food Security Program (GAFSP), which will help countries develop comprehensive plans to address agriculture and food security – two underlying factors that must be addressed in order to improve household resources for addressing child undernutrition.
The Committee on World Food Security (CFS) underwent a reform process throughout 2009. The reform document sets forth its commitment to broader participation by food security stakeholders and also unequivocally states that nutrition is integral to the concept of food security and to the work of the CFS. Finally, the United States Agency for International Development recently announced its Feed the Future initiative, which merges agriculture, health, and nutrition efforts and will spend at least US$3.5 billion to support countries such as Ethiopia, Guatemala, Nepal, and Rwanda in developing country investment plans for improving agriculture, reducing poverty, and improving nutrition.
The United Kingdom Department for International Development also recently launched its new nutrition strategy that sets out to tackle the “neglected crisis of undernutrition” by focusing on a set of immediate and long-term actions to reach children during the critical 1,000 days from conception to two years of age (DFID 2010).
The Hunger Task Force Report, which lays out the Government of Ireland’s priorities for reducing and eliminating hunger, also includes as one of its three focus areas the implementation of programs focused on maternal and infant undernutrition. The other two focus areas involve increasing the productivity of smallholder farmers – mainly women – in Africa and ensuring real political commitment at all levels to give hunger the absolute priority it deserves (Government of Ireland 2008).
Taken together, these new global efforts are a good beginning. Nonetheless, for global efforts to reach vulnerable populations and achieve the ultimate goal of well-nourished children, decisive and large-scale policy actions must ultimately be taken at national and subnational levels. Despite the scientific consensus on the importance of early childhood nutrition, the translation of research findings into actual policy and practice has been slow in many countries.
Developing country policymakers, even those concerned with devising policies to improve the well-being of their citizens, often neglect the nutrition of young children – their country’s future. The successes of countries that have made concerted efforts to prioritize nutrition should set an example for others that lag behind. The success stories, although diverse in the specific modalities and instruments used to tackle undernutrition, rely on a few common principles: strong government action coordinated across sectors and at central, state, and local levels; strengthening of existing health systems; significant scaling up of public spending; leadership and commitment at all levels; focus on and empowerment of vulnerable populations, households, and age groups; and a strong monitoring and evaluation culture that provides a basis for incentives and correction of policy actions in the context of implementation (von Braun, Ruel, and Gulati 2008).
By doing too little to address the crisis of undernutrition, policymakers are missing an opportunity to greatly improve the life prospects of millions of their citizens and thereby contribute to meeting broader policy goals on hunger, poverty, and economic growth.